This was calculated on a set of patients receiving a minimum of 30L of flow and 100% FiO2. They were aiming for O2 saturations > 92%. The study also found that the median duration of those who did well on HFOT was three days and those who did not do well, tolerated HFOT for about one day.
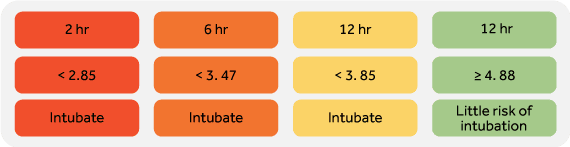
After Roca et al. carried out this study, they looked at the ROX index again and in 2019, carried out a prospective observational cohort study over 2 years this time[6]. The authors found that a ROX less than 2.85, less than 3.47, and less than 3.85 at 2, 6, and 12 hours of HFOT initiation respectively, were predictors of HFOT failure and that the ROX index was better than looking at SpO2/FiO2, RR, PaCO2, flow, SpO2, FiO2, and lactate to predict the need for mechanical ventilation; cementing further the need to use such an index.